I am a healthcare professional in the UK
I am a healthcare professional in the UK
 I am a patient or member of the public
I am a patient or member of the public
![]() 5 minutes
5 minutes
LIVTENCITY (maribavir) is indicated for the treatment of cytomegalovirus (CMV) infection and/or disease that are refractory (with or without resistance) to one or more prior therapies, including ganciclovir, valganciclovir, cidofovir or foscarnet in adult patients who have undergone a haematopoietic stem cell transplant (HSCT) or solid organ transplant (SOT).1
Consideration should be given to official guidance on the appropriate use of antiviral agents.1
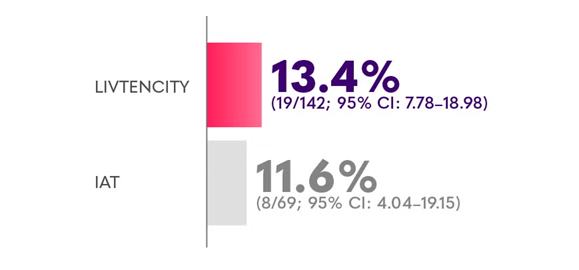
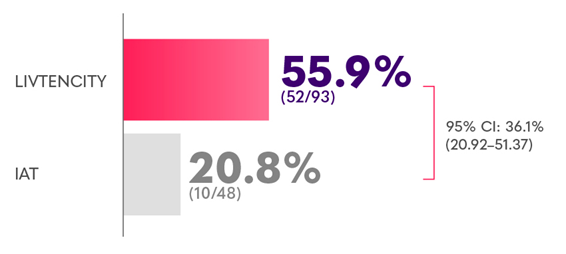
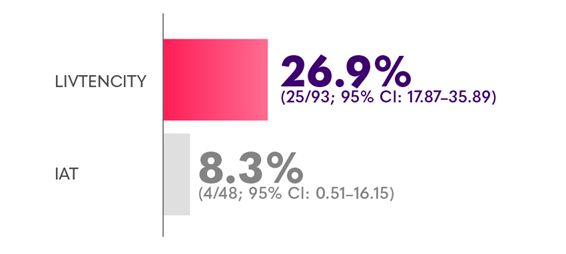
In the pivotal Phase 3 trial, LIVTENCITY delivered viraemia clearance of 18.7% at Study Week 8 maintained through Week 16 - almost double the proportion of patients compared with IAT (10.3%) - key secondary endpoint2
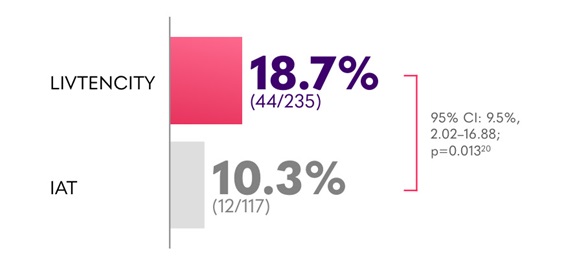
*Plasma CMV DNA <137 IU/mL in 2 consecutive tests ≥5 days apart.2
†CMV infection symptom control was defined as resolution or improvement of tissue-invasive disease or CMV syndrome for symptomatic patients at baseline, or no new symptoms for patients who were asymptomatic at baseline.2
*Limitations: This study was not powered to detect differences between treatments in this patient subgroup.2

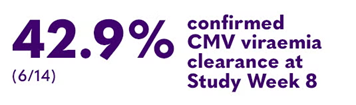
In a subgroup analysis of heart transplant recipients with refractory CMV receiving LIVTENCITY (6/14; vs 11.1% [1/9] on IAT)4
95% Cl: 30.7% (-1.72–63.2)

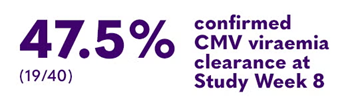
In a subgroup analysis of lung transplant recipients with refractory CMV receiving LIVTENCITY (19/40; vs 13.6% [3/22] on IAT)4
95% Cl: 38.2% (16.9–59.5)

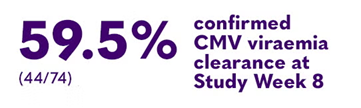
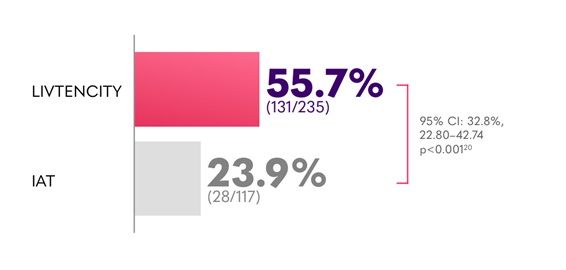
In a subgroup analysis of kidney transplant recipients with refractory CMV receiving LIVTENCITY (44/74; vs 34.4% [11/32] on IAT)4
95% Cl: 26.7% (7.5–45.9)


In a subgroup analysis of liver transplant recipients with refractory CMV receiving LIVTENCITY vs 0/1 on IAT5
Note: this subgroup analysis has been calculated from low patient numbers and the two treatment groups are not equally matched; therefore, it is insufficient to show a difference in treatment effect.
*Limitations: This study was not powered to detect differences between treatments in this patient subgroup.2
†CMV infection symptom control was defined as resolution or improvement of tissue-invasive disease or CMV syndrome for symptomatic patients at baseline, or no new symptoms for patients who were asymptomatic at baseline.2
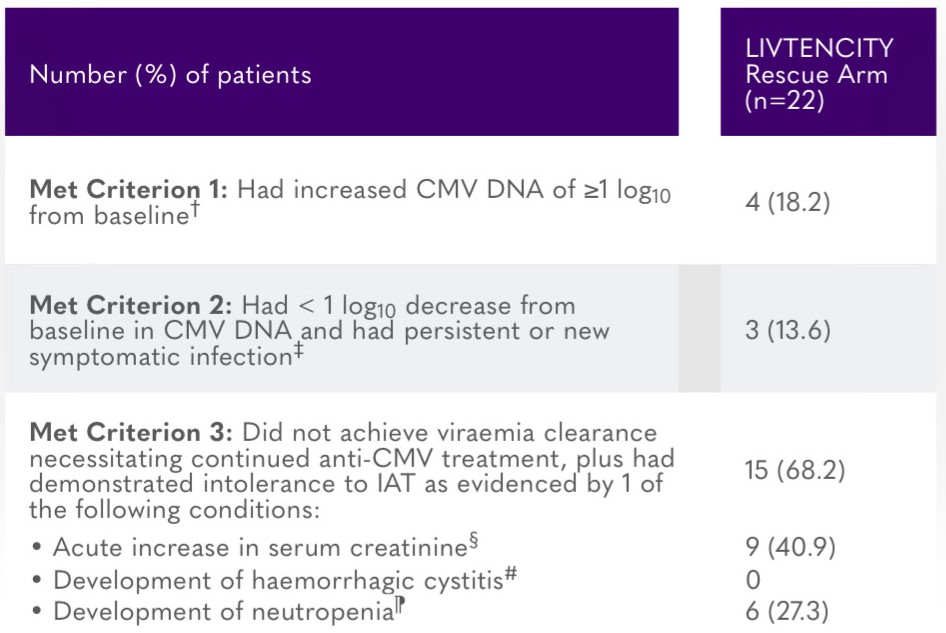
*All patients who entered the LIVTENCITY rescue arm had demonstrated persistence of CMV viraemia despite treatment with IAT for at least 3 weeks. All patients entered the rescue arm between study Weeks 3–7, except for 1 patient who entered between Weeks 7–8.7
†Whole blood or plasma CMV DNA levels were measured by local or central specialty laboratory qPCR assay.7
‡Patient had to meet 2 criteria: (i) whole blood or plasma CMV DNA had decreased <1 log10 from baseline as measured by local or speciality laboratory qPCR assay, and (ii) the presenting tissue-invasive CMV disease for symptomatic patients had not improved/worsened, or patient was asymptomatic at baseline and developed tissue-invasive disease.7
§At least 50% increase from baseline value, attributed to treatment toxicity (e.g. cidofovir, foscarnet).7
#When on treatment with cidofovir or foscarnet.7
¶Absolute neutrophil count <500/mm3 when on treatment with valganciclovir/ganciclovir.7
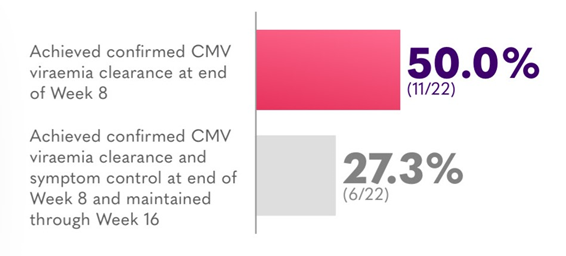
**Included all patients who entered the rescue arm and received any dose of LIVTENCITY as rescue therapy.7
Confirmed viraemia clearance = plasma CMV DNA < lower limit of quantification (i.e. <137 IU/mL) in 2 consecutive tests ≥5 days apart.2
IAT = one or a combination of ganciclovir, valganciclovir, foscarnet, or cidofovir.2
Refractory CMV = failure to achieve >1 log10 decrease in CMV DNA level in whole blood or plasma after a 14-day or longer treatment period with intravenous (IV) ganciclovir/oral valganciclovir; IV foscarnet, or IV cidofovir.2
Cl = confidence interval; CMV = cytomegalovirus; HSCT = haematopoietic stem cell transplant; IAT = investigator-assigned therapy; qPCR = quantitative polymerase chain reaction; SOT = solid organ transplant.


This concise guide to LIVTENCITY® (maribavir) is designed for clarity and ease of use. It summarises key insights from the Phase 3 SOLSTICE trial, including efficacy outcomes, safety data, and practical dosing guidance.

![]()
![]() 6 minutes
6 minutes
A summary of the safety profile of LIVTENCITY, including adverse event data and tolerability findings from clinical studies.

![]()
![]() 3 minutes
3 minutes
CMV is one of the most common infections experienced by transplant recipients
![]()
![]() 4 minutes
4 minutes
An overview of the pivotal Phase 3 SOLSTICE trial, outlining the study design, patient population, and methodology that underpin the clinical evidence for LIVTENCITY.





 1 minute
1 minute